Professional Orthodontist, ENT and Pediatrician Organizations Also Reject Trendy Sleep Apnea Treatments Touted By "Airway Dentistry"
A 2026 American Association of Orthodontists white paper concluded that no orthodontic intervention; including expansion; has been shown to prevent sleep-disordered breathing, and expansion alone does not reliably reduce apnea severity. The AAO further emphasizes that sleep-disordered breathing is a medical condition requiring physician diagnosis; orthodontists play a role in screening and referral, not independent diagnosis or airway-based treatment planning. Similarly, the AAO concludes that childhood extractions do not increase the risk of getting OSA and breathing problems in future.
I am writing this blog in continuation of my previous blogs on sleep apnea and airway dentistry; this time after an endorsement of my position by the American Association of Orthodontists (AA0).
A small section of dentists is marketing procedures like frenectomy and palatal expansion to treat, or prevent, sleep apnea, headaches, and TMJ problems. It sounds intuitive; make the airway bigger and improve breathing. But obstructive sleep apnea (OSA) is not simply an anatomic deficiency but a dynamic, sleep-state physiologic disorder. Static airway measurements; especially from dental cone-beam CT (CBCT) scans taken while a patient is awake and upright; do not reflect what happens during sleep. CBCT airway measurements are not considered valid for diagnosing or assessing treatment outcomes in sleep-disordered breathing.¹,² The AAO further emphasizes that sleep-disordered breathing is a medical condition requiring physician diagnosis; orthodontists play a role in screening and referral, not independent diagnosis or airway-based treatment planning. Similarly, the AAO concludes that childhood extractions do not increase the risk of getting OSA and breathing problems in future.
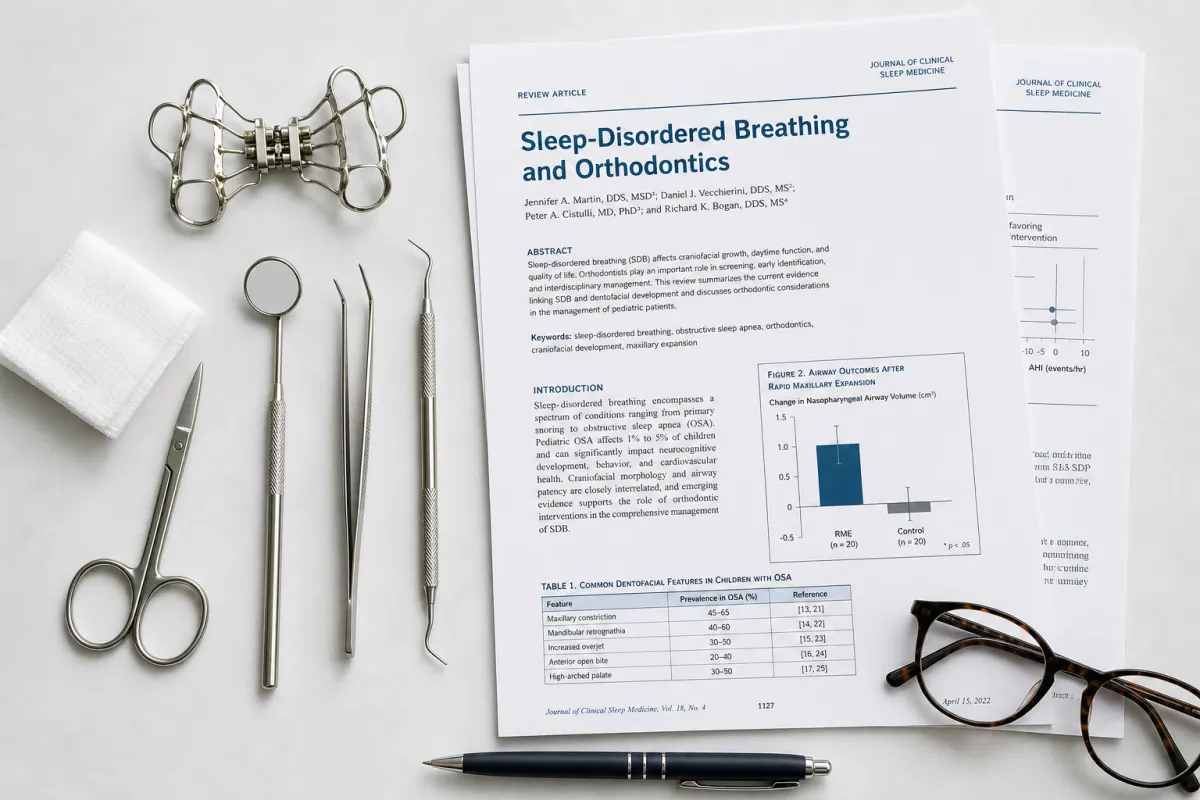
Palatal expansion is a well-established orthodontic treatment for transverse discrepancies; however, its role in sleep apnea is limited and often exaggerated. A 2026 American Association of Orthodontists white paper concluded that no orthodontic intervention; including expansion; has been shown to prevent sleep-disordered breathing, and expansion alone does not reliably reduce apnea severity.¹,³ When improvements are seen in children, they are typically in combination with medical interventions like adenotonsillectomy or reflect natural growth over time; not a stand-alone dental solution.⁴ There is also no evidence supporting prophylactic expansion to “prevent” future airway problems.¹ The same document notes that craniofacial anatomy like narrow palate and narrow lower jaw, cannot reliably predict sleep-disordered breathing; strong enough evidence does not exist to correlate narrow jaws with future airway problems.
Frenectomy has taken an even more dramatic leap; from a niche procedure with clear indications to a catch-all “airway solution.” While it may be appropriate in select infants with feeding issues, its use for sleep apnea, TMD, or generalized “airway optimization” is not supported by evidence. The American Academy of Otolaryngology states that ankyloglossia or tongue-tie does not cause sleep apnea,⁵ and the American Academy of Pediatrics cautions against extrapolating infant feeding data to unrelated conditions like OSA.⁶ The AAO further emphasizes that current evidence does not support routine frenectomy for the prevention or treatment of sleep-disordered breathing.¹
Recent consensus statements and evidence reviews from the American Academy of Dental Sleep Medicine and Journal of the American Dental Association (JADA) conclude that emerging dental therapies; including expansion and soft-tissue procedures; lack sufficient evidence to be considered first-line treatments for OSA.⁷,⁸ By contrast, treatments like CPAP and mandibular advancement devices have demonstrated measurable improvements in apnea outcomes and remain the standard of care.⁹
I reiterate again that a narrow jaw anatomy may matter for tooth crowding, but it is not always a pathological risk for sleep apnea and TMJ problems. Enlarging an airway on a dental scan does not mean improving breathing during sleep. Procedures like frenectomy and palatal expansion should not be marketed as solutions for complex medical conditions without strong evidence.
Recently, a new patient sought me out after reading my prior blogs on these topics. This blog is dedicated to that unnamed patient. If I ever decide to cross over to the other side of “airway dentistry,” I suspect I could finally justify upgrading my 2024 Toyota RAV4 Hybrid.
References
Palomo JM, Cohen-Levy J, Flores-Mir C, et al. Sleep-disordered breathing and orthodontics: an American Association of Orthodontists white paper update. Am J Orthod Dentofacial Orthop. 2026;169(4):419-427.
Savoldi F, Dagassan-Berndt D, Patcas R, et al. The use of CBCT in orthodontics with special focus on upper airway analysis in patients with sleep-disordered breathing. Dentomaxillofac Radiol. 2024;53(3):178-188.
Yu M, Ma Y, Xu Y, et al. Orthodontic appliances for the treatment of pediatric obstructive sleep apnea: a systematic review and network meta-analysis. Sleep Med Rev. 2023;72:101855.
Magalhães MC, Normando D, Soares CJ, et al. Impact of adenotonsillectomy and palatal expansion on apnea-hypopnea index: a crossover randomized controlled trial. Pediatr Pulmonol. 2024;59:3507-3517.
Messner AH, Walsh J, Rosenfeld RM, et al. Clinical consensus statement: ankyloglossia in children. Otolaryngol Head Neck Surg. 2020;162(5):597-611.
Thomas J, Bunik M, Holmes A, et al. Identification and management of ankyloglossia and its effect on breastfeeding in infants. Pediatrics. 2024;154:e2024067605.
Simmons M, Sheats R, Meira e Cruz M, et al. Emerging dental therapies for sleep disorders: evidence synthesis from the American Academy of Dental Sleep Medicine. J Am Dent Assoc. 2026;157(1):10-19.
Sheats R, Masse JF, Levine M, et al. Novel therapies for preventing and treating obstructive sleep apnea and snoring. J Dent Sleep Med. 2024;11(2).
Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea with oral appliance therapy. J Clin Sleep Med. 2015;11(7):773-827.
